










Aspadol 200 mg for Sciatica Pain – Dosage Guidelines & Real‑World Results
Explore Aspadol 200 mg (tapentadol ER) for sciatica relief. Learn about its dosage, effectiveness, side effects, and patient experiences in this guide.
1. Introduction
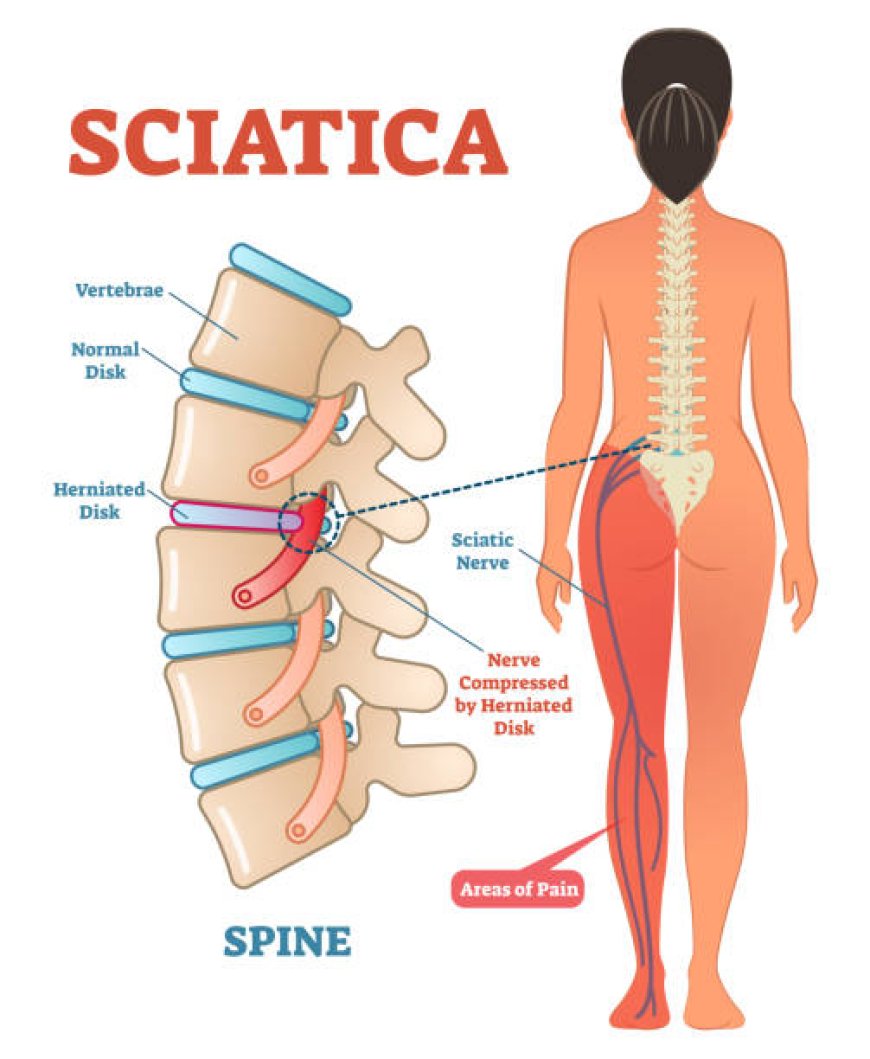
Sciatica lower backnerve painthatrunsdown the leg impactsmillionsglobally.Burning, tingling, or sharppain are frequent descriptors,andthisconditiongreatly affectsquality of life.NSAIDs, physiotherapy, and neuropathicmedications are first-line therapies. Aspadol 200?mg (tapentadol extended-release) is a Schedule?II opioid with atwo-prongedmechanism?-opioidagonismplusinhibition ofnorepinephrine reuptakeeffective for mixed nociceptive/neuropathic pain. This guidereviewswhether and how it works for sciatica,supportedby research, dosingstrategies, real-worldevidence, and safetyfactors.
2. How Tapentadol Works in Sciatica
Tapentadol's dual-actionprovidestheidealcombination:
-
?-opioid agonist:Suppressesascending pain signals.
-
Norepinephrine reuptake inhibitor (NRI):Potentiatesdescending pain inhibition pathwaysimportantin neuropathic painsuchassciatica.
Thiscombinationis supported byanopenpain trial thatreportedefficacyin more neuropathic profiles andincreasedquality of life.
3. Clinical Evidence in Sciatica & Low Back Pain
Direct sciatica trials arenot common,butlargestudiesofchronic low back pain with neuropathicfeaturesfrequentlyinvolvingsciaticaareinformative.
3.1 Phase IIIb Tapentadol PR Study
In 175 patients with mixed (neuropathic + nociceptive) low back pain, including sciatica, tapentadol PR (50250?mg BID)decreasedpain by 2.43.0 points on the NRSduring6 weeks (p?<?0.0001), withpainreliefsustainedduring 7 weeks ofconsistentdosing.
Thiswasmatchedbyreductionsin patient-reported neuropathic symptoms (e.g.,lowerfrequency ofpain attacks) inpatientswhowerehighscorerson painDETECT.
3.2 Opioid Conversion Study
Another open-labeltrialdemonstratedtapentadol ERequalledorexceededpotentopioidssuchasoxycodone inanalgesiaforopioid-switchedStep IIIpatientswithfewerGIadverseevents.
3.3 Systematic Review
In42 RCTsonchronic moderate-to-severe pain, tapentadolcausedmorepain reduction than oxycodone andalleviatedconstipation, nausea, and vomiting.
4. Real-World Patient Feedback
Qualitative Sciatica Pain Study
Inspiteofsideeffect concern, a pilot study of patientsondifferentmedications for sciaticareportedthatmostfoundtreatmentsineffective ordifficulttoendure.
Reddit Experiences
Patients report varying responses:
I do, I take Nucynta ER and it is hands down the best narcotic for neuropathy Im nearly pain free.
These echo clinical findings: tapentadol helps manyespecially in nerve pain contexts.
5. Recommended Dosage for Sciatica Pain
5.1 Extended-Release Regimen
-
Start: 50100?mg ER once or twice daily.
-
Titrate gradually (every few days) to effect, up to 250?mg BID.
-
Max daily: 500?mg (combined ER+IR)
5.2 Breakthrough Pain
-
Use IR 50?mg as needed (max 2/day, ?4?h apart).
-
Ensure total 24h dose ??500?mg.
5.3 Monitoring & Titration
-
Begin in 5 mg increments or 50?mg steps.
-
Assess relief, function, side effects after 12 weeks, then monthly.
6. Expected Results for Sciatica Pain
6.1 Pain Reduction & Quality of Life
-
Clinical studies show 23-point reduction on pain scales within weeks.
-
Responders often experience fewer pain episodes and better mobility.
6.2 Consistency & Tolerability
-
ER dosing offers ?12-hour steady relief, reducing nerve pain flare-ups.
6.3 Tolerability Advantages
-
GI side effectslike constipationare significantly lower compared to oxycodone CR.
-
Improved adherence and lower discontinuation rates are common.
7. Managing Side Effects & Safety
Common Side Effects
-
Nausea (30%), dizziness (24%), somnolence (15%), constipation, dry mouth.
Serious Risks
-
Respiratory depression when combined with alcohol or sedatives.
-
Seizure risk in predisposed individuals.
-
Serotonin syndrome with SSRIs/SNRIs/MAOIs.
Side Effect Management
-
Take with food; use stool softeners/laxatives.
-
Hydrate and monitor vitals during dose changes.
-
Screen for mood shifts or withdrawal symptoms.
8. Tapering and Discontinuation
-
Short-term (<4 weeks): may stop without tapering.
-
Long-term: slowly decrease dose by ~1025% weekly to prevent withdrawal.
-
Watch for anxiety, chills, insomnia; consider psychological support or MAT.
9. Safety Precautions & Contraindications
Avoid or be cautious in:
-
Severe respiratory disease, head trauma, or impaired liver/kidney function
-
Use with sedatives or serotonergic medications
-
History of seizures or substance misuse
Special care needed for elderly patients and those using multiple CNS drugs.
10. Comparison with Other Treatments
| Treatment | Sciatica Relief | GI Side Effects | Neuropathic Relief | Dosing Frequency | Abuse Risk |
|---|---|---|---|---|---|
| Tapentadol ER (200?mg) | High | Moderate (lower) | Yes (NRI included) | BID | Moderate |
| Oxycodone/ Morphine ER | High | High | No | BID | High |
| Gabapentinoids (e.g., preg) | Moderate | Edema, dizziness | Yes | Multiple daily | Low |
| SNRIs (e.g., duloxetine) | Moderate | Nausea, insomnia | Yes | Daily | Low |
| NSAIDs | Mildmoderate | GI/renal risks | No | Multiple daily | None |
Tapentadol ER stands out for its dual-action in nerve pain, making it more versatile than opioids alone, but carries higher risks than non-opioid options.
11. FAQs
Q1: How soon will tapentadol ER work for sciatica?
A: Relief usually begins within 12 hours; peak pain reduction is often seen by 34 weeks.
Q2: Is 200?mg ER strong enough?
A: Yes, 100250?mg ER BID is effective; 200?mg is a mid-range dose for many patients.
Q3: Can it cure sciatica?
A: Noit alleviates pain but doesnt fix issues like disc herniation or nerve compression. Physical therapy still essential.
Q4: What if I don't respond?
A: If pain persists after proper dosing, alternative neuropathic agents (e.g. duloxetine, gabapentin) may be needed.
Q5: Can I drive on it?
A: Avoid until youre confident in your responsedrowsiness and dizziness are common early on.
12. Final Thoughts